Sleep is often one of the first casualties of trauma. People living with post-traumatic stress often tell me they feel stalked by the night. Instead of drifting into rest, they brace themselves for the next nightmare, the next jolt awake, the next battle with their own mind. Many veterans arrive in my office surviving on two to four hours of broken sleep. The rest of the night is spent tossing, sweating, and bracing for dreams no one should have to revisit.
It gets worse. A strong body of research shows that behavioural treatments for fear reduction depend on healthy sleep in the nights following therapy sessions. When the brain does not get this recovery time, gains made in the clinic often fail to transfer fully into real life (Pace-Schott, Germain et al. 2015). In other words, disrupted sleep fuels trauma, and trauma fuels disrupted sleep. It becomes a vicious loop.
It is no surprise that people with PTS become desperate for rest. The usual advice about caffeine, screens, and bedtime routines often barely touches the sides in the early stages of recovery.
Many people then turn to sedatives such as Valium or Cannabis Products. When someone is frightened of sleep itself, the pull of medication makes complete sense. These medicines can act as a short-term circuit breaker, especially when anxiety about sleep becomes part of the problem. They can also help during acute spikes of stress.
Longer-term, however, sedatives often create more problems than they solve. Tolerance builds. Withdrawal worsens anxiety and insomnia. Alcohol and recreational drugs fall into the same trap. They may knock you out, but they disrupt the delicate architecture of healthy sleep that restores the nervous system.
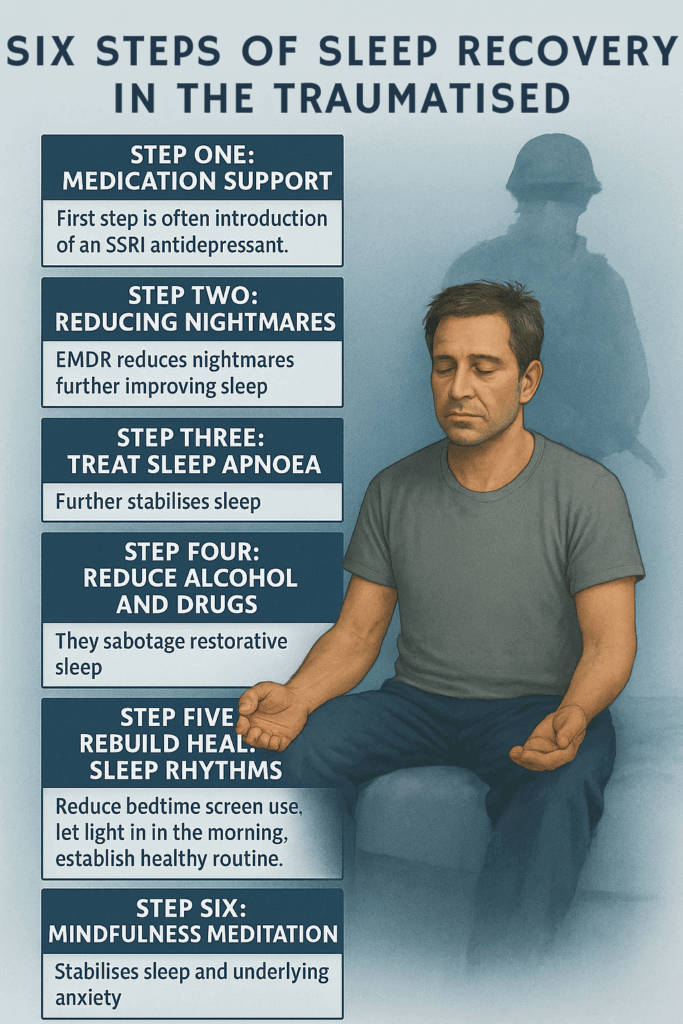
After many years working with trauma survivors, I have noticed a consistent pattern in how sleep recovers. It usually unfolds in six steps.
Step One – Initial Calming with Medication
The introduction of an SSRI antidepressant often settles baseline arousal. Many veterans move from shattered two-hour nights to something closer to four hours with fewer awakenings.
Step Two – Reducing Nightmares
When EMDR or related therapies reduce nightmares, sleep deepens further. Four hours of solid sleep is often followedrugsd by one or two lighter hours. It is not perfect, but it is meaningful progress.other drugs
Step Three – Reducing Alcohol and Other Drugs
Alcohol and other drugs sabotage sleep and interfere with emotional learning. Cutting back also improves sleep apnoea, which leads directly to the next step.
Step Four – Treating Sleep Apnoea
Sleep apnoea is often missed when nightmares dominate the picture. A partner’s observations are often the best starting point. Treatment, including CPAP, not only improves sleep but strengthens the extinction of fear-based memories (Reist, Jovanovic et al. 2021).
Step Five – Resetting the Body Clock
Once the earlier steps are in place, standard sleep hygiene begins to work. Regular routines, avoiding caffeine, protecting the bedroom as a screen-free space, and using natural timekeepers such as morning light, meals, and social contact all help stabilise circadian rhythm.
And then something softer begins to happen. Sleep improves gradually, like a shy creature gaining trust.
Step Six – Mindfulness Meditation
Mindfulness meditation now has strong evidence for improving insomnia in the general population (Rusch, Rosario et al. 2019) and supports trauma recovery once the worst symptoms have settled. Even mindfulness apps such as Calm show measurable benefits (Huberty, Green et al. 2019). Mindfulness quietens fear circuits and helps the body relearn that rest is safe.
For Residual Anxiety and Insomnia
Yet many people still report residual anxiety and light, unsettled sleep even when these steps are in place. This is often where transgenerational trauma enters the picture. Trauma does not always begin with us. Family history can live on as vigilance in the nervous system, tension in the body, and wakefulness at night.
This is where Mindful Representation work ( a very grounded form of Family constellations) can be transformative. By gently acknowledging the family stories the body still holds, people often experience a level of settling that standard therapy alone never quite reached. When inherited burdens loosen, sleep often follows.
Other Novel Therapies
There is also emerging evidence for light therapies. Green light (Zalta, Bravo et al. 2019), broad-spectrum white light (Youngstedt, Kline et al. 2022), and blue light (Vanuk, Pace-Schott et al. 2022) all show early promise as drug-free adjuncts.
Summary
Recovery from trauma is rarely linear.
Medication calms the storm.
Nightmare work restores the night.
Reducing alcohol clears the fog.
Treating apnoea restores oxygen.
Mindfulness teaches the body to trust.
Mindful Representation untangles what was never yours to carry.
If you are struggling with sleep after trauma, it is not a personal failure. It is your nervous system doing its best to protect you with the tools it learned long ago. Be patient. Be gentle. Healing happens in layers. Sleep returns in layers. And in time, night can become a friend again.
References
Pace-Schott, E. F., Germain, A., & Milad, M. R. (2015).
Sleep and REM sleep disturbance in the pathophysiology of PTSD: The role of extinction memory. Biological Mood & Anxiety Disorders, 5(3).
https://doi.org/10.1186/s13587-015-0018-9
Reist, C., Jovanovic, T., et al. (2021).
Sleep-disordered breathing and fear extinction retention in adults with trauma-related disorders. Journal of Traumatic Stress, 34(1), 57–67.
https://doi.org/10.1002/jts.22606
Rusch, H. L., Rosario, M., Levison, L. M., Olivera, A., Livingston, W. S., Wu, T., & Gill, J. M. (2019).
The effect of mindfulness meditation on sleep quality: A systematic review and meta-analysis of randomized controlled trials. Annals of the New York Academy of Sciences, 1445(1), 5–16.
https://doi.org/10.1111/nyas.13996
Huberty, J., Green, J., Glissmann, C., Larkey, L., Puzia, M., & Lee, C. (2019).
Efficacy of the mindfulness meditation mobile app “Calm” on sleep disturbance and depression symptoms in adults: Randomized controlled trial. JMIR mHealth and uHealth, 7(5), e13926.
https://doi.org/10.2196/13926
Zalta, A. K., Bravo, M., Valdespino-Hayden, Z., Augenstein, K., Otis, R., & Hunt, J. (2019).
A placebo-controlled pilot study of green light exposure for sleep in veterans with PTSD. Behavior Research and Therapy, 118, 109–118.
https://doi.org/10.1016/j.brat.2019.04.009
Youngstedt, S. D., Kline, C. E., Elliott, J. A., Zielinski, M. R., Devlin, T. M., Moore, T. A., & Burks, S. V. (2022).
A pilot study of intensive broad-spectrum light therapy for post-traumatic stress disorder. Journal of Psychiatric Research, 149, 190–196.
https://doi.org/10.1016/j.jpsychires.2022.02.019
Vanuk, J. R., Pace-Schott, E. F., et al. (2022).
Blue light exposure and sleep-related outcomes in individuals with post-traumatic stress disorder: A randomized controlled pilot study. Sleep Health, 8(4), 383–391.
https://doi.org/10.1016/j.sleh.2022.04.006